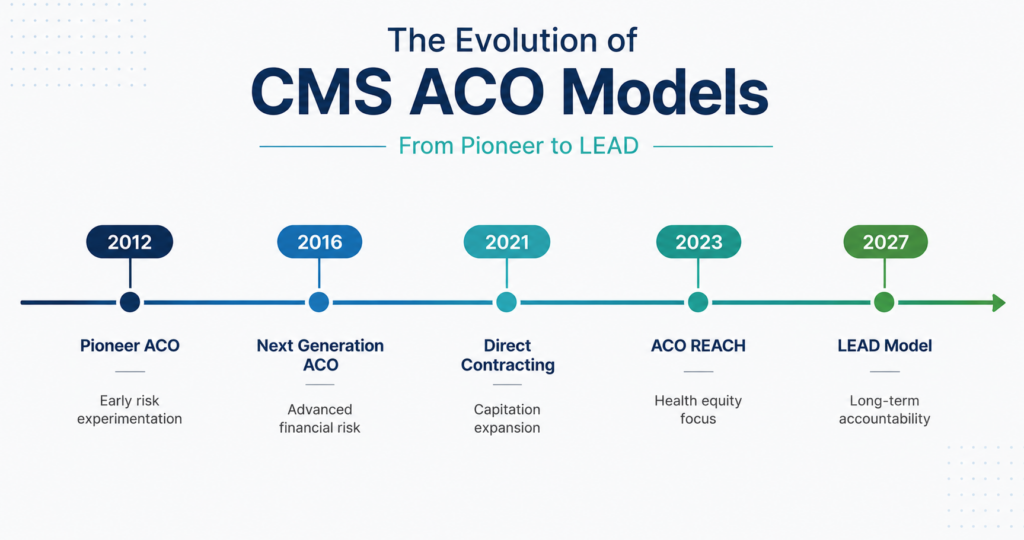
As the Center for Medicare and Medicaid Innovation (CMMI) prepares to launch the Long-term Enhanced ACO Design (LEAD) Model in 2027, we wanted to take a look back at the previous models.
But first off, if you are interested in applying:
The first LEAD application window closed May 17, 2026, at 11:59 p.m. ET. Organizations not ready to apply in the first cohort can submit a non-binding Letter of Interest by the same deadline. Application checklist with link to apply: https://www.cms.gov/priorities/innovation/files/lead-app-checklist.pdf
As a quick refresher for any of those who may be unfamiliar:
Under the CMS Quality Payment Program (QPP), providers can participate in one of two tracks.
- Merit Based Incentive Program (MIPS)
- Alternative Payment Models (APMs)
Inside the APM track, there are two main ACO families.
- Medicare Shared Savings Program (MSSP) – the permanent, statutory ACO program that’s been running since 2012. Serves 511 ACOs and more than 12.6 million Medicare beneficiaries
- CMMI models – time-limited experiments designed to test more aggressive payment structures
MSSP uses the APP Plus Measure Set, which replaced the APP Quality Measure Set. Our blog last year covers those changes – https://dynamichealthit.com/post/introducing-the-app-plus-quality-measure-set/
REACH and LEAD have their own measure sets, and while most of the reporting requirements from REACH carry over, there are two new eCQMs.
A Quick Recap
Pioneer ACO Model (2012-2016)
Aptly named, Pioneer was the first ACO model CMMI tested, and one of only 4 models CMMI has ever certified for expansion.
Starting with 32 ACOs and ending with 9, Pioneer tested whether established ACOs could handle capitation. Although 12 ACOs qualified for population-based payments in year 3, only 2 took them. In CMMI’s final evaluation report, they stated, “being at risk for losses while learning to manage the total cost of care under the rules of the Pioneer model and within a FFS context proved more difficult than anticipated.”
Next Generation ACO Model (NGACO) (2016-2021)
62 ACOs participated, with only 35 remaining by the final performance year. By introducing higher risk and reward, improved benchmarking, and tools to increase patient engagement, CMMI hoped to increase savings. While gross spending decreased by 1.9% over the 6 performance years, net spending remained unchanged, a now familiar pattern.
NORC, the independent evaluator, had some key insights in the final report.
- Specialty care belongs inside ACO models
- Population health takes time to pay off
- Lack of real time data and variations in EHRs limited care coordination
- No single factor was necessary for reduced spending
- Administrative burden and lack of financial predictability led to exits
Global and Professional Direct Contracting Model (GPDC) (2021–2022)
Launched in April 2021, GPDC introduced Direct Contracting Entities (DCEs) as a new structure. This model included three participant types (Standard, New Entrant, and High Needs) and two voluntary risk options:
- Professional – 50% savings/losses with one payment option, Primary Care Capitation Payment
- Global – 100% savings/losses with two payment options, Primary Care Capitation Payment or Total Care Capitation Payment
GPDC had three stated goals for the model:
- Transform risk-sharing arrangements in Original Medicare by tying payment to the quality of care provided to patients and reducing total expenditures through partially capitated payments that move away from traditional fee-for-service.
- Empower beneficiaries to engage in their health care with support from DCEs that help them to navigate the complex health care system. The model offered many additional flexibilities for beneficiaries, such as making in-home care management visits available when a patient is at high risk for hospitalization.
- Reduce provider administrative burden so that they could focus on what is most important: spending time with patients. For example, participants were able to report quality measures that focused more on outcomes and beneficiary experience in lieu of measures that focus on process. As a result, the providers could spend more time focused on the specific and individualized needs of their patients.
GPDC ran for only two performance years before CMS replaced it. Standard DCEs improved quality measures, but increased gross spending. New Entrants and High Needs DCEs did reduce gross spending. Across all three DCE types, net spending increased significantly after shared savings payouts. Higher risk levels were not associated with larger reductions in gross spending. 18 months into the model, it was redesigned into REACH.
On to the next one.
ACO Realizing Equity, Access, and Community Health (REACH) (2023-2026)
REACH kept the three ACO types and the same two risk-sharing options, but with strengthened governance, equity, and beneficiary engagement requirements. There were 132 participating ACOs in PY2023.
- Gross spending reductions reversed the GPDC trend, but cumulative net spending still increased.
- Across PY 2021–PY 2023, net spending across all ACO types increased by $1.1 billion once shared savings, losses, and performance bonuses were factored in. The familiar pattern persisted.
- Risk level and ACO structure
- ACOs electing Global risk with Total Care Capitation reduced spending, while ACOs electing Professional risk with Primary Care Capitation increased spending. ACOs structured as networks of individual practices reduced spending, while integrated delivery system and hospital-affiliated ACOs increased spending. This is the same IDS/hospital-system pattern that surfaced in NGACO and GPDC.
- Spending reductions were largest when
- Among Standard ACOs, the populations who needed care management most also showed the largest spending reductions: beneficiaries with eight or more chronic conditions ($588 PBPY), dual-eligible Medicare-Medicaid beneficiaries ($350 PBPY), and beneficiaries with disability or end-stage renal disease ($261 PBPY). This showed that advanced ACOs can deliver value for high-complexity populations.
- Quality improved across all three ACO types.
- All three reduced emergency department visits and observation stays without any decline in quality. Standard and New Entrant ACOs improved diabetes care and reduced hospitalizations for ambulatory care-sensitive conditions. High Needs ACOs improved timely follow-up after acute exacerbations and increased hospice utilization.
Long-term Enhanced Accountable Care Organization (LEAD) Model
While previous models proved ACOs can generate gross savings and improve quality, none have been able to reduce net spending. LEAD hopes to reverse the trend.
In previous models, successful ACOs faced benchmark rebasing that punished sustained performance. Small, rural, and physician-led practices couldn’t afford the infrastructure to participate. Hospital-affiliated ACOs underperformed their physician-practice peers. Specialists remained largely outside the accountable care framework. And quality measurement stayed claims-based.
LEAD is CMS’s attempt to address each of these. Per CMS, the model aims to “increase the scope of ACOs to include more small, more rural, and more independent health care providers and Community Health Centers,” enhance evidence-based prevention and care coordination, and empower patients to be more actively involved in their care.
Stable benchmarks for 10 years, no rebasing
Benchmarks update annually using a blend of prospective trend factors and observed national/regional spending, but the underlying baseline doesn’t get periodically reset. CMS describes this explicitly as creating “a pathway toward sustainable, long-term benchmarks and savings” so that “successful ACOs are not constantly having to exceed prior performance to share in savings.”
Support for high-cost ACOs
- Higher initial benchmarks for ACOs with historically high spending
- 1.5% Administrative Add-On Payment that helps high-cost ACOs with upfront cash flow
- Regional Efficiency Adjustment for low-spending ACOs in Global Risk
- Prior Savings Adjustment so ACOs that already generated savings in earlier models aren’t penalized
Lower alignment minimums for small and rural ACOs
- Standard ACO: 5,000 beneficiaries in PY1
- ACOs with >40% high-needs beneficiaries: 800 beneficiaries
- New ACOs: 1,000 beneficiaries
CMS Administered Risk Arrangements (CARA)
- Available only to Global Risk ACOs
- CMS-supplied infrastructure to negotiate episode-based risk arrangements with specialists
Episode types cover acute medical conditions (sepsis, respiratory infection, intracranial hemorrhage), chronic conditions (diabetes, heart failure, CKD, ESRD, asthma/COPD), surgical procedures, and a specialized falls-prevention episode called RISE (Resilience and Independence in a Safe Environment)
Quality withhold
REACH withheld 5% of the benchmark for quality performance. LEAD reduces that to 3%. Payments aren’t withheld during the year. At settlement, only the portion an ACO doesn’t earn back is applied against savings or losses. It functions more like a performance discount.
ACOs can earn back additional quality points by submitting a Prevention Quality Plan describing one prevention intervention tailored to their population (falls, diabetes, chronic disease).
Electronic Clinical Quality Measures
This is the change most relevant to the EHR and reporting side. GPDC and REACH relied entirely on claims data and patient surveys. LEAD introduces two electronic clinical quality measures (eCQMs):
Both are already on the MSSP APP Plus measure set, so most ACOs have seen them before. CMS phases eCQM reporting in over the first half of the model, ramping up after 2028. Four claims-based measures and CAHPS carry over from REACH.
- PY 1–2 (2027–2028): Optional (with 2.5 percentage point bonus per measure reported, on the Initial Quality Score)
- PY 3–4 (2029–2030): Pay-for-reporting
- PY 5–10 (2031–2036): Pay-for-performance
Continuous Improvement (CI) and Sustained Exceptional Performance (SEP)
“ACOs that meet or exceed predefined CI/SEP criteria could earn back all or a portion of their quality withhold based on their quality performance scores.”
Measure Comparison
| Measure | ID | Type | LEAD | ACO REACH | MSSP |
|---|---|---|---|---|---|
| Diabetes: Glycemic Status Assessment >9% | 122 | eCQM | ✓ | ✓ | |
| Controlling High Blood Pressure | 165 | eCQM | ✓ | ✓ | |
| Preventive Care: Depression Screening & Follow-Up | 134 | eCQM | ✓ | ||
| Breast Cancer Screening | 112 | eCQM | ✓ | ||
| Colorectal Cancer Screening | 113 | eCQM | ✓ | ||
| CAHPS Patient Experience Survey | Patient-reported | ✓ | ✓ | ✓ | |
| All-cause unplanned admissions for older adults with multiple chronic conditions | Claims-based | ✓ | ✓ | ||
| Risk-standardized all-condition readmission rates | Claims-based | ✓ | ✓ | ||
| Days at home for patients with complex, chronic conditions | Claims-based | ✓ | ✓ | ||
| Timely follow-up after acute events for certain chronic conditions | Claims-based | ✓ | ✓ | ||
| Clinician/Group Risk-Standardized Hospital Admission Rates (MCC) | Claims-based | ✓ | |||
| Hospital-Wide 30-Day All-Cause Unplanned Readmission Rate (MIPS) | Claims-based | ✓ |
Reporting population
LEAD requires eCQM reporting only for aligned Medicare beneficiaries, not all patients in a practice. That sounds like a relief, but most EHRs can’t natively filter measure logic to a CMS-supplied beneficiary list. ACOs will need to aggregate data across participant practices, filter to the aligned cohort, run the measure logic, and produce CMS-compliant output, the same way MSSP ACOs report under APP Plus.
Preparing for LEAD
- Decide on the application timeline. First cohort window closes May 17, 2026. Not ready? File a non-binding Letter of Interest by the same date.
- Audit your EHR’s eCQM capabilities. Can it filter measure logic to a CMS-supplied beneficiary list?
- Pilot CMS 122 and CMS 165 in 2027. Reporting is voluntary in PY 2027 and 2028 with bonus points available. Test extraction, calculation, and submission workflows before scoring matters.
- Build your Prevention Quality Plan. Identify one prevention intervention tailored to your population
- Engage vendors early. eCQM aggregation, CARA episode data, beneficiary-list filtering
How DHIT can help
If your organization is sorting out the data-aggregation side of LEAD readiness, DHIT can help with multi-EHR quality measure aggregation. Our CQMsolution product consumes QRDA I XMLs from any EHR, de-duplicates patient data, runs CMS-certified measure logic, and outputs CMS-ready submissions.
Will LEAD be able to balance paying ACOs enough to make participation worthwhile against capturing enough net savings to justify the program to taxpayers?