

The DHIT team recently participated in HL7 events that are helping shape the future of healthcare data interoperability, including the FHIR Connect-a-thon and WGM+ in our hometown New Orleans, LA.
Our participation in HIMSS, C-CDA IAT, FHIR Connect-a-thon, and the HL7 WGM+ has given us great insight to important knowledge and trends.
These working sessions served as a platform to share ideas between professionals from all parts of the world, with topics such as:
- C-CDA/USCDIv1-4/USCDI+
- USCore FHIR Resources
- CodeX HL7 FHIR Accelerator Program
- Subscriptions
- Quality Measures (Clinical Reasoning)
The HL7 FHIR Connect-a-thon and the Virtual HL7 Consolidated Clinical Document Architecture (C-CDA) Implementation-A-Thon (IAT) were two events that were crucial in advancing C-CDA and FHIR specification. These events brought together implementers and developers to hold technical discussions resulting in the development of FHIR-based solutions for data exchange.
HL7 FHIR Connect-a-thon
7 Years Participating in Clinical Reasoning Track
The HL7 FHIR Connect-a-thon was a two-day event held on May 6th and 7th. The event aimed to engage participants in testing their implementations of the FHIR Implementation Guides. Familiar faces, passionate discussions, great food and multiple perspectives was a reminder to all attending that FHIR is not only about patients but also about people.
Quality Measures and NCQA FHIR Collaboration
Last year DHIT engaged in a Pilot with NCQA FHIR-based Quality Measures. This was our first focus on Digital type Measures involving Claims and Clinical Data. DHIT is collaborating with teams from Mitre, The Joint Commission, NCQA, and other measure developers to ensure the roadblocks to the FHIR-based Quality Measure process are known and addressed.
We focused on the evaluation of EH measures 71, 104, and 506. We were able to successfully incorporate and test the latest versions of these measures. We are exploring the challenges of the volume of data and frequency of data element updates during a patient’s visit. The industry recognizes there are many challenges surrounding these aspects. We also incorporated the following into our FHIR server – CMS 72, 108, 190, 334, 506, 1028. as well as the EP measures 2, 50, 68, 129, 146, 177, 349, 819, 996. Our Team worked through testing these measures and shared our findings. We will be exploring future workflows for submission.
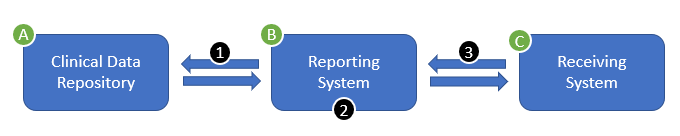
- Gather: The Reporting System queries the Clinical Data Repository for the data required to evaluate the measure
- Evaluate: The Reporting System evaluates the quality measure, producing a MeasureReport resource
- Report: The Reporting System posts the completed MeasureReport to the Receiving System
USCDI Evolution and Healthcare Interoperability
Currently, CMS is encouraging “collaboration with internal team, federal, and state partners, and the private sector to further specify and implement critical actions that will transform CMS’s quality measurement enterprise to be digital and overall reflect a healthcare ecosystem with nationwide interoperability.”
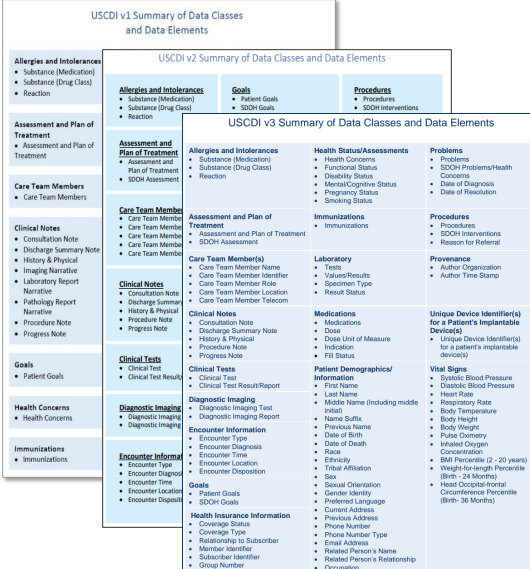
ONC continues to evolve the USCDI requirements for EHR data necessary to be interoperable using FHIR standards with the release of several USCDI versions, expanding the inventory of data elements that should be standardized. In addition, recognizing that USCDI will not be able to meet all unique medical specialty, agency or use case-specific data needs, ONC created the United States Core Data for Interoperability Plus (USCDI+), which will support additional datasets or extensions beyond what is captured within the base USCDI.
USCDIv2 and v3 Implementation
Since CMS & ONC have a Proposed Rule specifying USCDIv3 as the required dataset for Certified EHRs, DHIT is focused on supporting USCDIv2 & v3 data collection in the Dynamic FHIR API. With an eye towards future opportunities involving our niche EHR vendor partners, we are closely following the ONC’s USCDI+ initiative to define specialty or program-specific data extensions to USCDI.
We recognize EHR vendors will have a transition period regarding moving data to FHIR, so we are concurrently continuing efforts to parse QRDA I documents to FHIR.
To ensure successful engagement within the FHIR community, it is imperative for those involved to attend WGM task meetings regularly. These sessions offer a great opportunity for seasoned teams and newcomers alike to share and exchange knowledge about their progress. On our team, we have members who are responsible for USCDIv2, SDOH, C-CDA to FHIR mapping. We are also ramping up our efforts to build quality measures with the help of experts in the field.
Implementation-A-Thon Recap
The IAT was held in April and was also a two-day virtual event. The objective of the IAT was to expand outreach to engage new communities and increase the impact of this content improvement effort which offered Tracks for hands on collaboration.
At the C-CDA IAT our team worked directly with the taskforce and collaborated with other EHRs. Our work here involved helping assure C-CDA Payer section interoperability. We discussed payer/coverage differences – between group and plan – that need to be addressed, as FHIR has two separate sections for these concepts which require an extension for customization.
Our extensive work will influence future Companion Guides to ensure payer data can be included in the CCD and parsed to FHIR.
Multiple DHIT team members attended various tracks and sessions such as “C-CDA Templates for specialty data use cases” and “Unhappy Documents – Review of C-CDA documents that are not well structured or easy to use”.
C-CDA Templates for specialty data use cases: Specialty Group, Optometry Track
Gathering insights directly from providers (or ex-providers) has been invaluable in understanding how certain changes must be implemented in real-life settings. With the help of one of our Strategic Partners we have a better understanding of topics like the refracturing process, data entry at a patient encounter level, connections between the C-CDA, and so on. During this research period, we’ve dedicated much of our attention to optometry while gaining applicable knowledge that can be used for other specialties or general use cases.
Unhappy Documents – Reviewing Poorly Structured C-CDA Documents
This was an opportunity to work with colleagues in our field and discuss how a discharge summary document can be helpful to streamline patient transition. We gained useful insight into how the Implementation Guide (IG) will need to be restructured and approved by relevant governing bodies.
Future Collaboration Opportunities
Our expertise and the knowledge gained through industry collaboration ensure DHIT continues to be a part of successful integration with industry leaders and software.
Any EHR vendor, consumer, or implementor looking to improve the C-CDA document outputs or address data needed in C-CDA should consider joining the next virtual C-CDA IAT, August 23 & 24 and consider suggesting a topic.