We continue waiting with bated breath for the 21st Century Cures Act Final Rule. In the past, the HHS Office of National Coordinator (ONC) has enjoyed the fanfare of announcing new rules at major conferences, but that was not the case during the recent ONC’s 2020 Annual Meeting. The 21st Century Cures act was passed with wide bi-partisan support in December of 2016. The Proposed Rule has been out for nearly a year now. Apparently it is still stalled in review at the Office of Management and Budget (OMB).
Nevertheless, there was a lot of activity at the conference and some interesting initiatives for interoperability in healthcare that continue to move forward.
Some highlights:
HHS Secretary Alex Azar was delayed due to urgent high-level discussions with Chinese government officials and others about the Corona (not to be confused with the beer) virus. When he spoke, though, his message was a powerful one regarding information blocking,
“Glad to speak at the ONC 2020 Annual Meeting this morning. Patients need and deserve control over their records; interoperability is the single biggest step we can take toward that goal.”
He also said “Scare tactics are not going to stop the reforms we need” – apparently taking a shot at Epic’s threatened lawsuit.
Patients’ rights to their data and empowering patient data access were perhaps the most common examples of interoperability in healthcare. These topics were discussed by many participants from various perspectives. The discussion that most resonated with me was Grace Cordovano’s impassioned plea for patients and patient advocates’ access to their electronic health records.

She is “boots on the ground” with cancer patients and cited not
only onerous processes of gathering paper records and “driving across borders to get CDS” but also talked about how receiving a “life-altering, life-limiting diagnosis” totally changes a patient’s perspective re. privacy vs. access. Once they’ve received such a diagnosis, they are driven to “acts of survival.” In general, she sees patients asking “What’s happening with my data? What are you going to do with it?”
The “Congressional Perspective on Unique Patient IDs” plenary session was an interesting one and dovetailed into the patient rights conversation. Congressman Bill Foster (IL-11) is the author of the amendment to repeal the ban on unique patient IDs. As a PhD physicist and inventor in addition to being a politician, Dr. Foster presented a well-reasoned argument for moving forward with unique patient IDs. Some key points:
- Until recently, many insured people were afraid of losing their healthcare benefits due to pre-existing conditions if their medical history was able to follow them. Of course, this is no longer an issue since the onset of Obamacare.
- Real ID and TSA Pre-Check have been surprisingly popular.
- With the Opioid Crisis, it is becoming increasingly important to ID patients in a foolproof way and this isn’t limited to curbing “Doctor shopping” by addicts. Congressman Foster cited a real-life example of a recovered addict who was inadvertently given opioids during emergency medical treatment and then subsequently relapsed and died.
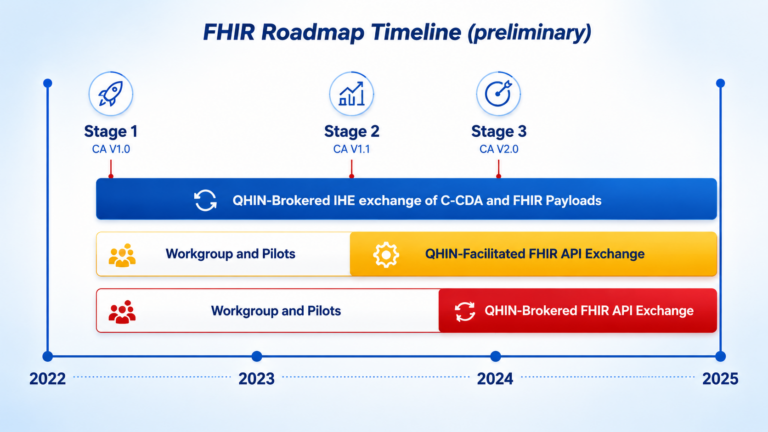
As always, in recent conferences, FHIR integration was front-and-center. Almost every speaker mentioned FHIR and there was even a panel discussion “Measuring the Uptake and Use of FHIR® to Advance Interoperability”. We are still waiting, though, to see which version of FHIR ONC mandates with the Final Rule!
Of particular interest to us here at DHIT was NCQA’s presentation about “Digital Quality Measures”. We have expertise with Electronic Quality Measures (eCQMs) and calculating eCQMs directly from EHR data. Digital Quality Measures expand on this concept by taking it a step forward – continue to use EHR data but combine it with data from other sources such as HIEs, claims and elsewhere without regressing to a manual abstracting process. This is an excellent use case for Unique Patient IDs!